




ICU Management & Practice, Volume 18 - Issue 1, 2018
As has been pointed out, the benefits of tight glycaemic
control in the ICU have by no means been clearly established or accepted. In
2010 a meta-analysis of seven prospective randomised studies concluded that
intensive insulin therapy in mixed ICU patients was not supported by evidence.19
Today we understand that hyperglycaemia, hypoglycaemia, and high glycaemic variability are all associated with poor outcomes. A review of 44 studies in the literature reporting hyperglycaemia in over 500,000 ICU patients found an association with many different types of outcomes. Another study on a large database of more than 100,000 patients, demonstrated that hyperglycaemia, hypoglycaemia, and high glycaemic variability all increased the risk of in-hospital mortality.20
Another large multi-centre study in 45,000 ICU patients found
that while hyperglycaemia, hypoglycaemia, and high glycaemic variability were
each independently associated with mortality, diabetic status modulated these
relations such that patients with diabetes may benefit from higher target
glucose ranges than those without diabetes.21
What therefore is the best way to manage blood glucose in the ICU?
The digestion and absorption of carbohydrates is a complex
sequence of events starting in the mouth with amylase, which breaks starches
down into shorter-chain sugars. Dextrins and sucrose are broken down further by
specific enzymes, while other enzymes (lactase and maltase) at the brush border
of the gut contribute to the breakdown of lactose and the oligosaccharides. The
end result is glucose, which passes into cells and is released into the
bloodstream.
The different types of dietary carbohydrate, such as
monosaccharides, oligosaccharides, or polysaccharides, differ in their speed of
absorption. The “glycaemic index” is used as a convenient classification to
categorise the speed of absorption.
Regarding enteral nutrition, some diabetes-specific formulas
(DSF) are available, which are characterised by a lower percentage of
carbohydrates and a higher percentage of lipids than standard formulas.
However, rather than the amount of carbohydrate, the key difference is the type
of carbohydrate as the formulations are put together to give a lower glycaemic
index for the diabetes-specific formulas.
A systematic review of the literature in this area included RCTs which compared DSFs with standard formulas, finding that DSF was more effective in controlling glucose profiles. The requirement for insulin in patients with diabetes was lower when using these DSFs.22 The authors speculated that this may be due to the type of carbohydrate used in these formulations, which may be more slowly digested and absorbed than in standard formulas.
There are not many studies on the role of DSF in the ICU. A
small study of DSF in hyperglycaemic, mechanically ventilated, critically ill
patients assigned around 50 patients to each of three groups, two of which used
DSFs while the third used a standard control formula.23Insulin requirements were lower in the two DSF groups, while
glycaemic control was significantly better.
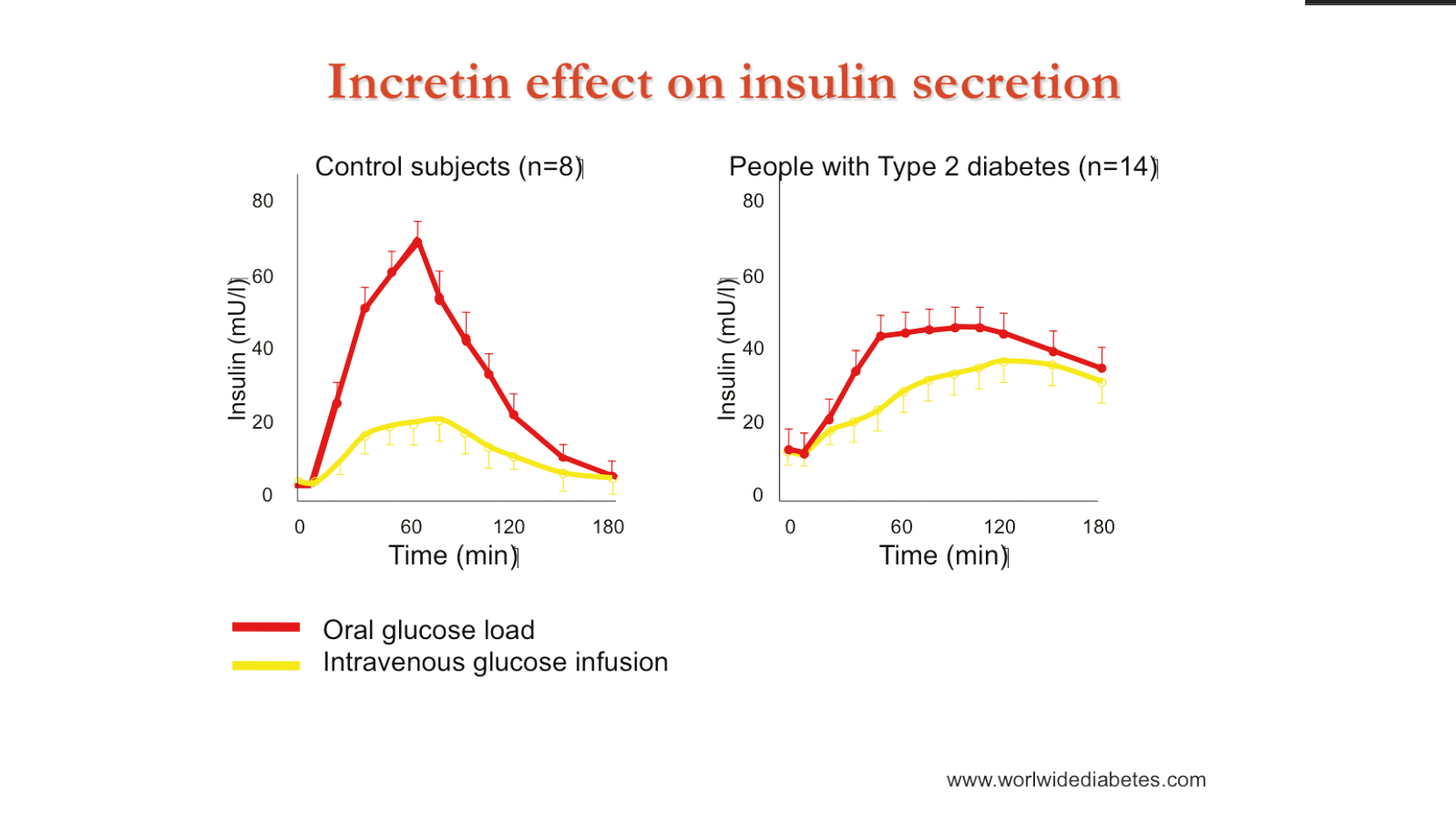
An important physiological issue that we have to consider in
feeding critically ill patients is the incretin effect. Following oral feeding,
hormones released by the GI tract will stimulate the pancreas to release
insulin. In healthy, non-diabetic subjects, administration of glucose by the IV
rather than oral route results in the stimulation of much lower quantities of
insulin, as the gut hormones are not produced in the same quantities. In
diabetic patients, there is very little difference between the two routes of
administration.
A meta-analysis of 13 studies examining the influence of
enteral vs parenteral nutrition on glucose control in patients with acute
pancreatitis confirmed that PN was associated with an increased risk of
hyperglycaemia and therefore an increased requirement for insulin.24
In patients receiving continuous enteral feeding, if this is associated with a release of endogenous insulin then the amount of exogenous insulin needed to maintain a steady blood glucose level would be lower during feeding and higher during interruptions. Hence, the calculated insulin sensitivity would fall when feeding is interrupted and rise when feeding is restarted.
This hypothesis was tested in a group of critically ill,
non-diabetic patients for whom records were available, for a minimum of 10
hours of enteral feeding followed by at least 7 hours with an interruption to
enteral feeding, and at least 5 hours of resumed EN.25 Data for 52 of these patients was available and it was found
that insulin sensitivity dropped following interruptions to enteral feeding,
thereby supporting the presence of an incretin effect.
New guidelines for glucose control were published in 2010
just after the controversy between the Leuven studies and the NICE-SUGAR study.26Unfortunately these guidelines reflect the uncertainty and
lack of evidence: regarding carbohydrate intake it is not possible to suggest a
general recommendation of maximal or minimal amounts of intravenous or enteral
carbohydrates to be administered to critically ill patients regardless of the
type, the severity of the pathology and the delay from onset of disease. It is
also suggested that hyperglycaemia be reduced by restricting intravenous
glucose in critically ill patients.
A pragmatic approach is to begin EN as soon as possible,
adapting the infusion rate to the tolerance of the patient, trying to limit
caloric debt rather than to achieve full matching of energy expenditure. In
some centres, routine clinical practice includes the administration of low
doses of IV glucose (50-100g/day) as a maintenance solution. As well as this,
the use of dynamic scales for the dosing of insulin and attempts to minimise
glycaemic variability are strongly recommended.
References:
20. Badawi O. Crit Care Med 2012;40:3180-8.
21. Krinsley JS. Crit Care 2013;17:R37.
22. Ojo O. Nutrients 2014;6:5142-52.
23. Mesejo A. Crit Care 2015;19:390 doi: 10.1186/s13054-015-1108-1.
24. Petrov MS. Clin Nutr 2007;26:514-23.
25. Jamaludin UK. e-SPEN, the European e-Journal of Clinical Nutrition and Metabolism 2012:e154-9.
26. Ichai C. Crit Care 2010;14:R166.
